- Visibility 149 Views
- Downloads 6 Downloads
- DOI 10.18231/j.ijodr.2024.040
-
CrossMark

Growth modulation with maxillary expansion appliances-A review
Introduction
The ideal way to treating malocclusion with jaw discrepancy in children is to modify facial development. Correcting malocclusion requires effective treatment of skeletal issues. Several orthopaedic and functional appliances can be used to modify growth in the transverse, vertical and sagittal planes. Skeletal Class II may result from retrusion of the mandible, protrusion of the maxilla or a combination of the two. Any skeletal issue can be treated with orthodontic surgery, growth manipulation, and dental concealment. To optimize treatment outcomes through growth modification, it is recommended that patients with Class II malocclusions begin therapy at the onset of cervical vertebral maturation stage CS3. The treatment age ranges from 8 to 14 years old. [1]
Class III malocclusion is best described by disparities between the skeletal and dental components in the vertical or antero-posterior axes. Skeletal Class III malocclusion typically manifests clinically as retrognathic and narrow maxilla, prognathic and broader mandible or a mix of both. When skeletal issues arise, maxillary transverse deficit is the first dentofacial dimension to stop growing. The mid palatal suture, like all cranial sutures, becomes more twisted and interdigitated as people age, hence prompt repair is necessary.The use of functional appliances for growth modulation has generated a lot of discussion. Correct diagnosis, case selection, appliance selection, and patient compliance are likely the most important aspects in its success. Three expansion treatment modalities are used today: rapid maxillary expansion, slow maxillary expansion and surgically assisted maxillary expansion. The type of malocclusion, the patient's age, and the dentition's developmental stage are taken into consideration when choosing the appliances. [2], [3] This review explains various methods used in maxillary and mandibular expansion.
Discussion
Growth modulation with maxillary expansion appliance
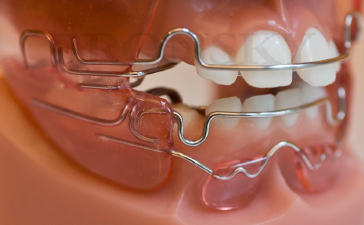
Functional Regulator(FR), developed by Rolf Frankel, aids in the passive expansion of dental arches when used in conjunction with fixed appliances([Figure 1]). Because the special vestibular shields of the FR appliance are constructed 3 mm from the maxillary mucosa, arch expansion and posterior lower tooth up righting are both passively enabled. The growing teeth can passively straighten and enlarge in the maxilla because the forces produced close to the surrounding mucosa are kept at a distance from them. The principle author saw the clinical outcomes of FR treatment in 1975 and again in 1979 when he went to Frankel’s clinic in East Germany. [4] Assessing 75 patients using the serial dental model that is currently available and the data from the two clinical visits, it was possible to achieve consistent extension of the dental arches over the long term. Following two patient-centered clinical studies using Frankel’s regulator and the concurrent implementation of rapid maxillary expansion as a standard clinical procedure, the author started investigating the potential for both orthodontic and orthopaedic expansion in growing individuals, with a particular emphasis on the stability of dental arches expansion over the long and short term. [5]
Rapid maxillary expansion(RME)
The most common application in orthodontic treatment is rapid maxillary expansion, or RME. The upper jaw expands most quickly when the expansion appliance is used at a rate of 0.5–1 mm/day, or two quarter turns of the screw/day, or twice a day([Figure 2]). In two to six weeks, there is a quick correction of the cross-bite due to rapid maxillary expansion(RME). There could be a formation of midline diastema, indicating the mid-palatal split. The diastema would naturally shut as a result of the gingival fibers stretched trans-septal group recoiling.[5], [6] A desirable clinical practice is a slight over-expansion of the maxilla where the lingual slopes of the maxillary lingual cusps touch the mandibular buccal cusps. This over-expansion makes allowance for the relapse particularly of the buccal tipping of the molars. [7]
During orthodontic treatment with RME, the mid-palatal suture opening accounted for 12%-52.5% of the total screw expansion. The mid-palatal suture appears to undergo recalcification following RME treatment, indicating that its expansion is stable. The results of this comprehensive study did not consistently support the hypothesis that the mid-palatal sutural aperture was triangular or parallel. Different responses can be seen in the osteogenic response in the enlarged mid-palatal suture and the orthodontically induced osteogenesis in the PDL of neighboring incisors. While the nearby extended suture underwent bleeding, necrosis, and a wound healing response, the widened PDL directly induced the formation of new bone. Vascular invasion of the blood clot in the expanded suture is a prerequisite for new bone formation. [8]

Indications for RME
An absolute narrow maxilla, a difference between the maxillary and mandibular first molar and premolar widths of at least 4 mm.
Class III malocclusion with narrow maxilla/pseudo-Class III of dental and skeletal in nature
Nasal stenosis combined with a narrow maxilla
Severe case of many teeth in cross-bite
A quick expansion is the preferred method when the maxillary molars are buccally inclined, since a traditional dentoalveolar expansion will tip them farther into the buccal musculature. The mandibular molars may exhibit lingually inclined dentoalveolar compensations in a different scenario involving a small maxilla. Cross-bite and the requirement for maxillary skeletal growth would arise from an attempt to position the mandibular dental segments on the skeletal basis.
When compared to an untreated control group RME in the early mixed dentition seems to be a successful technique for increasing the rate of eruption of palatally misplaced maxillary canines(65.7%).
Contraindications for RME
Subjects with convex profiles, steep mandibular planes, and anterior open bites are typically not treated with RME. For RME therapy, an increased mandibular plane angle is not a strict rule.
Age. When the midpalatal suture has undergone synostosis, it is the top age limit. Adjunctive surgery, however, overcomes this.
Inadequate anchoring support is caused by poor periodontal health
A normal state for this type of face is one in which the mandible and maxilla are both constricted.
Design of RME
RME devices can be classified into bonded or banded appliances based on how they are placed in the mouth. The banded expansion appliance is connected to teeth using bands located on the maxillary first molars and first premolars. Hass's initial RME design suggested adding an acrylic cover to the palatal vault. This appliance design was rejected because of the challenge in maintaining cleanliness, especially on the palatal side. As a result, the wire framework hygienic expander or HYRAX appliance was brought into use. Banded appliances are not suitable for use in deciduous and early mixed dentition.[9] The different appliance design consists of a wire framework and acrylic components that aid in securing the appliance. Individuals with high FMA also show similar design of RME appliance. Extending occlusal acrylic over buccal surfaces can help minimize molar extrusion. This device is especially beneficial in Class II situations, as the extraction of molars would lead to a backward and downward movement of the jaw, which would increase the facial convexity and the vertical dimension of the lower face. [10] The bonded maxillary expansion device helps correct anterior cross-bite in Class III young patients by creating a bite block effect. The fixed appliance design can also be utilized in the adult teeth due to its convenient handling process and various beneficial clinical outcomes. The necessity for putting on and taking off separation elastics, adjusting bands, transferring into alginate impression, bending precision wire, and soldering is no longer required. [9], [10]
Cemented hygienic rapid expansion (HYRAX) appliance
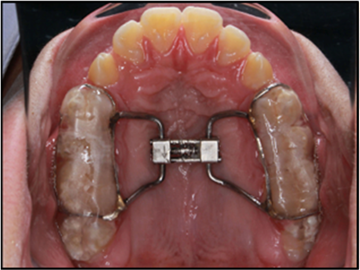
The critical design of the cemented HYRAX appliance requires the acrylic plate to cover the teeth crowns, with only 1 mm of space at the gingival margins on the buccal and palatal sides([Figure 3]). This ensures that there is enough space at the gingival line for maintaining good oral hygiene and the ideal coverage for retention. Acrylic extensions with chamfer finishes have a lower food lodgement. It is not necessary for acrylic occlusal covering to be thicker than 1-2 mm, and it should have holes drilled into it to allow any excess cement to be released. Modern glass ionomer cement significantly improves cemented expander retention, obviating the necessity for acrylic or composite-based materials that require acid-etching processes. The screw should be positioned as high in the palatal vault as is practical, regardless of the type of device. With the thread axis aligned with the front edge of the first permanent molars, the screw is positioned in the centre of the arch. [11]
Slow maxillary expansion(SME)
Upper jaw slow expansion is characterized as progressing at a rate of 0.5 mm per week. Every third day of the week, the upper removable appliance(URA) is scheduled to gradually expand by one-quarter turn (0.25 mm)([Figure 4]). Faster growth typically causes the device to move in the mouth. The degree of maxillary constriction determines how long the treatment will take. [12]
Palatal expansion screw
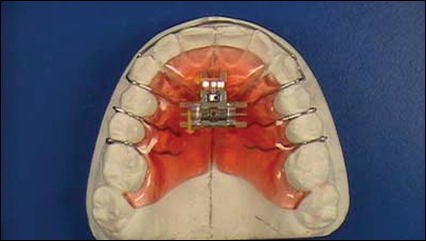
The expansion screw design of the maxillary expansion has an acrylic body with a parallel screw inside of it. The acrylic plate is separated in the middle of the palate, and clasps keep the appliance in place on the teeth. The palatal split and expansion screw are sealed with acrylic after the required expansion is attained( [Figure 5]). The identical device can serve as a retainer for a duration of 6 to 8 months. In certain situations, it may be necessary to have occlusal coverage in order to release occlusion and allow for expansion.[13]

Wire framework expander appliances
Wire frame maxillary expansion devices are primarily used to promote growth of the dental arch. The device can have a removable construction that slides into the inner sheets of the upper first or second molars, or it can be welded or soldered to the inside of the first molar bands. With its acrylic body, the coffin spring could be considered the oldest type of wire maxillary expander.[14]
Quad helix/tri-helix appliance
The quad helix appliance, a variant of Coffin's W-spring, was initially described by R.M. Ricketts as a treatment for patients with cleft palates who had significant collapse. The four helices on the W-spring improve its control over expansion, lengthen its activation range, and boost its flexibility. In cases of cross-bite, the palatal arms of the device can be adjusted to correct the needs of the arch. The quad helix device measures 0.038 inches in size. Depending on the patient's age, bands are joined to either the baby second molars or the first permanent molars in the upper jaw via stainless steel wire. In prepubertal children, the quad helix appliance functions through a mix of buccal tipping and skeletal expansion at a 6:1 ratio.[15] Chaconas et al. found that around 14 ounces of force is generated by an initial 8 mm expansion before cementation. This amount of force is enough to move teeth, but usually not adequate to cause orthopedic changes in adults with a closed mid-palatal suture. Yet, resistance at the patent suture is typically lower in children with deciduous or early mixed dentition compared to the dentoalveolar area. This device can expand the maxilla orthopedically in children([Figure 6]). [16]
The expansion was deemed sufficient as long as the maxillary lingual cusp made contact with the mandibular buccal cusp on both sides in centric relation. It is suggested to slightly overexpand by around 2-3 mm in order to account for the uprighting of the buccally tipped teeth after retention is stopped. The quad helix appliance is held in the widened yet relaxed position for a 6-week period once the proper expansion is reached. At times, the device may create a mark on the tongue. Nonetheless, this will quickly fade away once the appliance is taken out. [16], [17]
By removing the lateral forced bite, treatment with a quad helix appliance, which aims to extend the maxillary arch, creates ideal conditions for proper growth of the jaws, TMJ, and face. A systematic review indicates that 16% to 50% of individuals may have spontaneous correction of this issue in the absence of treatment. [4]
Nonetheless, the success rate with RME and the quad helix appliance is almost 100%. While occlusal grinding can be helpful, it is not always effective(27–90%), and expansion plates are significantly less effective(51%–100%). Premature deciduous tooth contacts can be removed to effectively stop a posterior cross-bite from continuing into the adult teeth and mixed dentition. Therefore, the most evidence-based form of therapy may not be the most effective one. Every case should receive individual attention based on the severity and nature of the issue, as well as ongoing monitoring. [18]

NiTi expander
The NiTi expander was introduced to the orthodontic profession by Wendell V. Arndt([Figure 7]). All stainless steel, including the lateral palatal arms, is used throughout the device, with the exception of its center component, which is constructed from a thermally activated NiTi alloy. By utilising the form memory and transition temperature of titanium, the NiTi is able to function. Activation of nickel-titanium expanders is not necessary once they are inserted into the lingual tubes. [19] The negatively rotated molars expand and derotate effectively simultaneously as a result of the activated device. The nickel titanium expander has a transition temperature of 94 °F. When it's cold before insertion, it may be twisted more easily and is more pliable. The expander starts to apply a gentle, constant push to the teeth and the mid-palatal suture as the mouth warms the appliance, metal stiffening and restoring from memory. A 3mm expansion increment only produces a force of roughly 360g. There are eight distinct intermolar widths for nickel titanium expanders, ranging from 26 to 44 mm, and they produce forces between 180 and 300g.
For younger patients, the softer wires in the 26–32 mm sizes result in lower force levels. The clinician assesses the required expansion and adds 3 mm for overcorrection to establish the proper size. Measuring the mandibular intermolar distance at the central fossa is an easy approach to figure out the right size. To get ready for lingual sheet insertion, the expander assembly can be wrapped with the freeze-gel packs that come with the expander kits. This will enable the device to cool down sufficiently for simple insertion into the lingual sheaths. To prevent heating the nickel titanium, the expander should be held by the molar attachments during insertion.[20] Slightly beyond the molar bands will be where the passive appliance is located. When the nickel titanium is distorted for insertion, it causes an initial activation that rotates the molars distally and expands the bicuspids and molars. Baccetti et al. noted improvements in the maxillary first molars mid-palatal rotation and posterior cross-bite. Dentoalveolar expansion and molar derotation are successfully achieved with the NiTi expander. When cleft patients show substantial molar rotation and anterior arch collapse, the author prefers to utilize the NiTi appliance. Mini-implant connected quickly to the palate. A hybrid hyrax, a mini-implant supported expander appliance is supported on both the tooth and the bone. The growing need for orthodontics among adult patients has led to a rise in popularity for the skeletal anchored expansion appliance, which can split the mid palatal suture in adults. [21], [22]

Alt-RAMEC
Liou created the Alt-RAMEC protocol, which effectively disarticulated teeth without excessively enlarging the dental arch([Figure 8]). This procedure mirrored distraction osteogenesis. Patients with or without clefts can utilize it. He employed a unique double-hinged expander, the placement of which allowed the maxilla to migrate forward more readily as the center of rotation was close to the maxillary tuberosity. The specialized hinge screw can alternatively be substituted with the Hyrax expander. For anterior displacement, double-hinged expanders have been shown to be superior to the other varieties. [15], [18]

According to the Alt-RAMEC protocol, maxillary expansion of one millimeter per day must be followed by seven days of maxillary constriction of one millimeter per day. Following a 7–9 week repetition of this cycle, the maxilla was lengthened using a traditional facemask with extraoral elastics or a fixed intraoral ®–Ti maxillary protraction spring. By moving the jaw downward and tilting the palatal plane upward, the ®-Ti maxillary protraction spring opens the bite. Therefore, it should not be used by those with an anterior open bite or a high mandibular plane angle. Using a ®-Ti maxillary protraction spring, it has been demonstrated that for growing patients with cleft lip and palate, the amount of maxillary protraction was 5.8 ± 2.3 mm in 3 months (2 months of Alt-RAMEC followed by one month of protraction) and two years later, the outcomes didn't change. Studies have shown that the maxilla migrates forward more when Alt-RAMEC and facemask therapy are used together than when the RME facemask method is used alone. Maxillary protraction does not need to wait for the completion of the Alt-RAMEC procedure. The facemask treatment can begin at the same time as the expansion regimen. On the other hand, it was said that the fast maxillary expansion group was more compliant than the Alt-RAMEC group. [23], [24]
Conclusion
In children maxillary expansion can achieve excellent dental and skeletal change. There are numerous ways to accomplish the expansion of upper jaw. The skeletal and dental pattern type mostly influences the type of expansion chosen, which can greatly facilitate the overall treatment objectives. Regardless of the types of expansion appliances used, many studies agree that maxillary expansion is a stable procedure that consistently achieves favorable short- and long-term outcomes. Growth modification's ultimate outcome is dependent on a number of factors, including the patient's quick compliance, desired dental and skeletal conditions, appliance functionality, treatment duration, and timing.
Source of Funding
None.
Conflict of Interest
None.
Acknowledgement
None.
References
- HJDe Clerck, WR Proffit. Growth modification of the face: A current perspective with emphasis on Class III treatment. Am J Orthod Dentofacial Orthop 2015. [Google Scholar]
- SN Rita, SA Sadat. Growth modification in Class II malocclusion: A review. Update Dent Coll J 2014. [Google Scholar]
- K Maruswamy, UA Nayak, PA Nayak, S Ramasamy. Management of class III malocclusion - a review with report of four cases. Ann of Dent Spec 2018. [Google Scholar]
- WR Proffit, HW Fields, BE Larson, DM Sarver. . Contemporary orthodontics-ebook 2019. [Google Scholar]
- JA Mcnamara, R Lione, L Franchi, F Angelieri, LHS Cevidanes, MA Darendeliler, P Cozza. The role of rapid maxillary expansion in the promotion of oral and general health. Prog orthodont 2015. [Google Scholar]
- CT Pavlick. Cervical headgear usage and the bioprogressive orthodontic philosophy. Semin Orthod 1998. [Google Scholar]
- FP Henriques, G Janson, JF Henriques, DC Pupulim. Effects of cervical headgear appliance: a systematic review. Dental press J Orthod 2015. [Google Scholar]
- A Agarwal, R Mathur. Maxillary Expansion. Int J Clin Pediat Dent 2010. [Google Scholar]
- E Yepes, P Quintero, ZV Rueda, A Pedroza. Optimal force for maxillary protraction facemask therapy in the early treatment of class III malocclusion. Eur J Orthod 20141. [Google Scholar]
- S Hata, T Itoh, M Nakagawa, K Kamogashira, K Ichikawa, M Matsumoto. Biomechanical effects of maxillary protraction on the craniofacial complex. Am J Orthod Dentofacial Orthop 1987. [Google Scholar]
- A Alammar. Difference in Pain Perception Between Banded and Bonded Hyrax during Rapid Palatal Expansion. Int J Dent Sci Res 2021. [Google Scholar]
- S Naidu, A Suresh. Slow Palatal Expansion a Novel Method of Arch Expansion. Guident 2019. [Google Scholar]
- RB Kuril, R Samuel. A novel approach for correction of tooth transposition. J Indian Orthod Soc 2012. [Google Scholar]
- NA Parkin, HF Mckeown, PJ Sandler. Comparison of 2 modifications of the twin-block appliance in matched Class II samples. Am J Orthod Dentofac Orthop 2001. [Google Scholar]
- RH Samuels, F Willner, J Knox, ML Jones. A national survey of orthodontic facebow injuries in the UK and Eire. Br J Orthod 1996. [Google Scholar]
- AH Owen. Crozat treatment. J Clin Orthod 1985. [Google Scholar]
- R Miralles, B Berger, R Bull, A Manns, R Carvajal. Influence of the activator on electromyographic activity of mandibular elevator muscles. Am J Orthod Dentofacial Orthop . [Google Scholar]
- MT Tung, M Makaremi, FDe Brondeau. Neuromuscular environment and stability of transverse maxillary expansion. J Dentofac Anomal Orthod 2017. [Google Scholar]
- S Williams, B Melsen. Condylar development and mandibular rotation and displacement during activator treatment: an implant study. Am J Orthod 1982. [Google Scholar]
- CM Forsberg, L Odenrick. Skeletal and soft tissue response to activator treatment. Eur J Orthod 1981. [Google Scholar]
- G Montaruli, M Laurenziello, LL Russo, C Chimenti, L Lo, D Ciavarella. Bilateral or Unilateral Cross-Bite Treatment with Nickel Titanium Palatal Expander (NPE-2) in Young Adults. J Dent Oral DisorTher 2016. [Google Scholar]
- W Clark. Twin-block functional therapy: applications in dentofacial orthopaedics (second edition). Am J Orthod Dentofac Orthop 2004. [Google Scholar]
- NG Toshniwal, PC Katkade, SA Mani. Fixed functional appliances. J Evol Med Dent Sci 2021. [Google Scholar]
- V Sitaropoulou, HN Yilmaz, BE Yilmaz, N Kucukkeles. Three-dimensional evaluation of treatment results of the Alt-RAMEC and facemask protocol in growing patients. J Orofac Orthop 2020. [Google Scholar]
- Introduction
- Discussion
- Growth modulation with maxillary expansion appliance
- Rapid maxillary expansion(RME)
- Indications for RME
- Contraindications for RME
- Design of RME
- Cemented hygienic rapid expansion (HYRAX) appliance
- Slow maxillary expansion(SME)
- Conclusion
- Source of Funding
- Conflict of Interest
- Acknowledgement