- Visibility 3k Views
- Downloads 72 Downloads
- Permissions
- DOI 10.18231/j.ijodr.2021.048
-
CrossMark

Abstract
Malocclusions need to intercepted at an early developing stage to prevent severe disturbing outcomes. In all reported cases, Class II is one of the most common malocclusions that is seen which requires treatment using functional appliances as it presents with considerable difficulty in later stages. Twin block has the advantage of versatility of appliance designs and they meet a wide range of requirements for correction of various types of malocclusions for patients. The aim of this study is to include all modifications that could be incorporated in the appliance design to be customized to individual patients according to their need.
Introduction
Malocclusions needs to be intercepted at an early developing stage to prevent severe disturbing outcomes. In all reported cases, Class II is one of the most common malocclusions that is seen which requires treatment using functional appliances as it presents with considerable difficulty in later stages. Class II malocclusion could be due to retrognathic mandible, prognathic maxilla or a combination, but retrognathic mandible has been more commonly observed.
Functional appliances have proven to be one of the most helpful in modulating growth of the craniofacial region in the growing stage of an individual. These appliances harness forces from the neighbouring musculature to produce skeletal and dental changes.
Twin block is a tooth and tissue borne appliances that links them to maximize the orthopaedic forces. Twin block in the treatment planning in orthodontics is the most accepted amongst functional appliances since it’s advent due to wide acceptance and as its aids in rapid treatment results, ability to perform normal oral functions without any hinderance and ability to be worn for long hours which further motivates the patient thereby increasing the patient compliance.
Twin block is widely used for class II Div.1 cases but modifications were made to adapt it to different sets of occlusions. Accordingly, a number of modifications that were incorporated in the conventional appliance design according to various malocclusions and is therefore customizable for individual needs.
It was made to achieve more skeletal changes as compared to the less desirable dental changes, especially observed that one of the major drawbacks is that the overjet correction during the treatment is largely due to Dentoalveolar changes so required changes are made to enhance the skeletal changes.
Twin block has the advantage of versatility of appliance designs and they meet a wide range of requirements for correction of various types of malocclusions for patients. [1]
The aim of this study is to include all modifications that could be incorporated in the appliance design to be customized to individual patients according to their need.
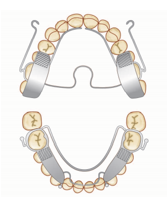
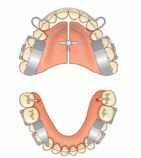
Standard twin blocks were designed with following components [1]
A midline screw to expand upper arch to accommodate the mandibular changes that are caused during the advancement.
Occlusal bite blocks are placed at a 70o inclined plane for mandibular advancement as it gives maximum advancement without causing much discomfort to the patients.
Delta clasps on upper premolars and molars to improve the fixation of twin block, these clasps are better suited to take up the forces without breaking that is required during the twin block treatment.
Ball end clasps mesial to lower canine or in upper premolar or deciduous molar region to improve the retention of the appliance.
A labial bow is incorporated in the upper arch if there are severely proclined incisors that require uprighting.
Twin block appliances are ideally simple bite blocks that are designed in such a way that they can be worn for 24 hours and therefore help in achieving rapid functional correction of malocclusion by transmitting the forces that are favourable to occlusal inclined planes that are build to cover the posterior segment. These forces which are transmitted through the dentition provides a constant proprioceptive stimulus that influences the growth and bone structure.
The underlying skeletal and soft tissue factors frequently affects the cuspal guidance and poor occlusal function, this unfavourable cuspal guidance may act as a deterrent to the growth of mandible and therefore are unable to attain its optimum genetic growth potential.
In a retrusive mandible, mandibular dentition does not offer the required support to the maxillary arch and affects the transverse maxillary development. The constriction of the width in the maxillary dentition thus enforces a locking effect causing a distal occlusion and therefore does not allow mandibular development.
Twin block in Class III cases
Reverse twin block [1]
Functional correction of Class III malocclusion in Twin Block technique is achieved by reversing the angulation of the inclined planes, thereby harnessing occlusal forces as the functional mechanism to correct arch relationships by maxillary advancement, while using the lower arch as the means of anchorage.
Reverse twin blocks are fabricated to enhance the maxillary development by action of the revere inclined planes that allows forward movement of upper teeth and at the same time restricts the development of mandible.
The maxillary appliance should include provision for three-way expansion to increase the size of the maxilla in both sagittal and transverse dimensions. It can be modified to be used in conjunction with Reverse-pull headgear. An initial stage of rapid maxillary expansion is often indicated to free up the maxillary sutures prior to applying forward traction to the maxilla (McNamara 1993).
They can also be used with lip pads to enhance forward movement of upper labial segment that gives an action similar to Frankel III.
The case selection of cases to be treated with reverse twin block is very critical. Early treatment is usually needed to counter the development of mandible that can be unfavourable to skeletal harmony. Orthopedic corrections are usually achieved by maxillary advancement rather than mandibular retraction as it is difficult to alter the growth potential of mandible except through surgical procedure.
The degree of discrepancy in the skeletal structures is one of the most important factors in case selection, when the convexity moves into the negative range the patient should be informed about the need for surgical procedure to achieve a stable occlusion. Reverse twin block can be effective in early mixed dentition stages but relapse is very likely to occur during the pubertal growth spurt which would then require intervention.

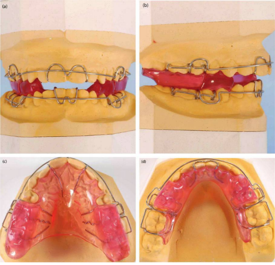
Modified twin block for class III with lip pads[2]
Class III is a rare malocclusion; it is easy to diagnose but challenging to treat. Many treatment approaches have been recommended in the past such as functional appliances like reverse twin block (RTB), Frankel III appliance, removable mandibular retractor (RMR), and orthopedic appliance like face mask. It was believed that rapid expansion along with lip pads can be added to reverse twin block so that it could yield more skeletal changes as opposed to conventional design.
The appliance included a hyrax screw adapted parallel to the occlusal plane; bite blocks were constructed at 70o to the occlusal plane configured in reverse to the conventional twin block. Wax relief was placed between wire extension for lip pads and model, these lip pads were rhomboidal in shape.
Other appliances that have proven to be effective in class III malocclusion are Frankel III appliance, removable mandibular retractor (RMR) and orthopedic appliances like facemask are proven to be effective. This appliance has a greater effect on maxillary advancement and much better control on the posterior positioning of mandible with minimal dental compensation.
Twin Block to Control Incisor Inclination in Class II Malocclusion
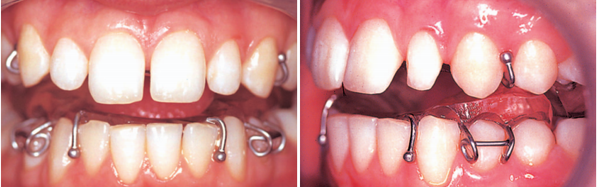
Modified twin block with torquing spurs [3]
Appliance design: Wire spurs passing around the upper incisor tips and up the labial surface
The reduction in incisor retroclination was statistically and clinically very significant as compared to appliances with labial bow
It was also observed that there was reduction in extrusion of upper incisor tip.
Skeletal changes showed nearly twice the reduction in ANB that suggested modest maxillary restraint and a slightly larger mandibular anterior change.
Modified twin block with torquing spurs and high pull headgear [4]
To control the vertical and sagittal growth of maxilla many authors have recommended the use of high pull headgear in combination of functional appliances that will allow the mandible to auto-rotate and increase its forward displacement. This appliance allows to maximize the skeletal changes whilst reducing the dentoalveolar changes in correction of malocclusion. Torquing spurs were added to the upper incisors in order to reduce the retroclination of the upper labial segment and the high pull headgear directed at the centre of resistance of maxilla was used in attempt to control the vertical positioning of the maxilla.
Appliance design: Maxillary components included Adams clasp on molars and premolars and torquing springs on central incisor, steep inclined plane with midline expansion screw and flying headgear tubes next to 2nd maxillary premolar and a high pull headgear with 400g per side force worn for 14-16hrs per day. Mandibular components included Adams clasp on molars and premolars and ball end clasps on incisors. The treatment was finished when full reduction in overjet and overbite and sagittal correction of posterior occlusion.
Dentoalveolar effects
Due to the use of torquing springs the retroclination was reduced to a certain amount but did not reach statistically significant value, there was slight evidence of significance with respect to increased distal movement of the maxillary molars.
Skeletal effects
It was observed that the maxillary plane had rotated in an anticlockwise direction shown by negative SN-palatal plane value but it was not statistically significant, it was concluded that since the headgear tubes were located next to premolars the value didn’t reach the desired amount and perhaps if the tubes were placed more anteriorly an increase in magnitude of anticlockwise rotation could have been achieved. It also caused increased in anterior relocation of pogonion as measured from articulare suggesting that it was more effective in correction sagittal class II discrepancy. There was no increase in Lower anterior facial height to total anterior facial height (LAFH/TAFH) ratio due to effective control of maxillary occlusal plane.

Modified twin block with Southend clasp on lower central incisors [5], [6]
The Southend clasp was originated by DiBiase and Leavis.It locks the tooth surface against the acrylic base plate providing greater control over the axial inclinations of the incisors. The design is similar to the original Jackson clasp. The southend clasp was given to get a better control over the lower incisors axial inclination which is of a great concern during the treatment of class II malocclusion.
This modification of the twin block design is done to achieve maximum correction of the malocclusion by skeletal changes and by reducing the amount of dentoalveolar component.

Modified twin block with Southend clasp on upper and lower central incisors [7]
In treatment of patients with class II div 1 malocclusion the overjet can be corrected by the retraction of dentoalveolar structure involving the upper incisors or by mandibular advancement. The twin block treatment involves both these mechanisms but it is beneficial to maximize the mandibular advancement for correction of the overjet which can be achieved by gaining control over the incisors by using southend clasps.
The presence of a Southend clasp reduced the level of upper incisor retroclination by almost half during Twin-block appliance treatment. An important secondary finding was that the presence of a Southend clasp reduced the amount of lower incisor proclination. There was also a small, but statistically significant enhancement in the skeletal correction, as measured by change in the ANB angle, in the Southend clasp group.
The use of a Southend clasp on the upper and lower incisors of a Twin-block appliance in carefully selected patients. The advantages of fabrication of such an appliance is that it reduces retroclination of the upper incisors; proclination of the lower incisors and also applies control to the incisors which may enhance the skeletal correction.
Modified twin block with acrylic capping [8]
According to Clark incisal capping was done to prevent incisor proclination during the functional therapy treatment but on further investigation it was seen that a 5-degree proclination occurs during the treatment without the capping but the incisors upright during the support phase and there is no proclination seen at the later stages.
At the tips of lower incisors there was decalcification seen where the acrylic capping was done and not a significant restrain was observed in incisor inclination.
The proclination of lower incisors was due to lingual appliance components while mandible attempts to rebound to normal resting procedure.

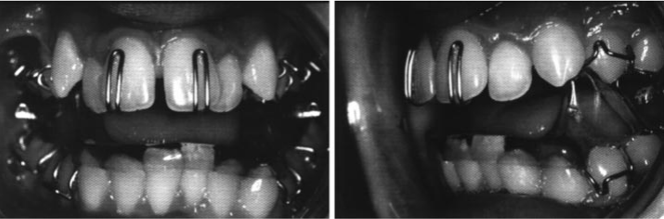
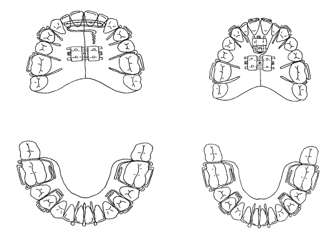
Modified twin block for class II Div 2 [9]
1) A double cantilever spring behind the upper labial segment (Figure), followed by bonding of the upper labial segment with pre-adjusted Edgewise fixed appliances;
2) addition of one anterior screw with torquing spurs to both upper central incisors (Figure).
There are obvious advantages such that treatment time may be significantly reduced by eliminating a pre-functional phase of treatment. As advancement of the upper labial segment occurs simultaneously with sagittal correction the patient should never have an increased overjet placing them at risk of trauma due to prominent upper incisors. This technique also prevents patients being left with an increased overjet if they fail to comply with the functional phase following upper incisor proclination. Various additions to the upper Twin Block are available for proclination of the upper incisors. In these two cases an anterior screw with torquing spurs on the maxillary central incisors and a double cantilever spring have been used. However, T or Z springs could also be used to provide this movement.
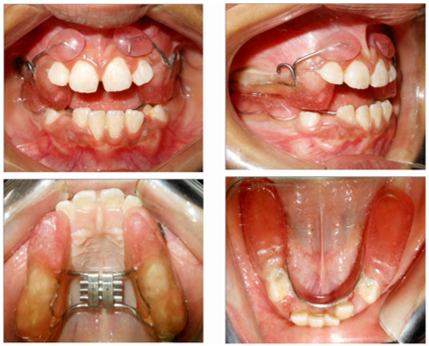
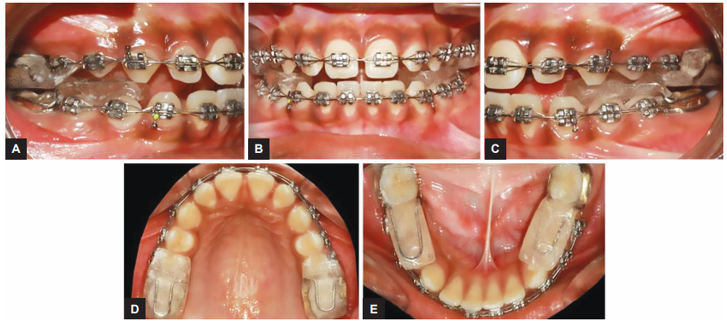
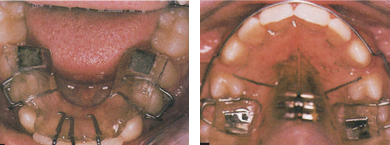
Modified twin block with mini implants [10]
Used in class II Div 1 case
Mini implants have been used in orthodontics since a long time. It has proven to be effective in reducing the unfavourable dentoalveolar effects by providing absolute anchorage from bone. Although use of mini-implants is a popular method of anchorage control in orthodontics but its use with twin block is not common. This method provides for a better control over the position of lower incisors in order to achieve maximum orthopedic correction in twin block therapy.
Appliance design: Maxillary components consist of delta clasps and labial bow while the mandibular components include delta clasps, ball end clasps, wire hooks projecting distal to canine on both sides, two mini-implants placed bilaterally between mandibular second premolar and first molar in aseptic condition and intraoral elastics were given of dimension 3/8” that were engaged to wire hooks and implants to exert class I distalizing force. The elastics were replaced daily. There was no change in position of lower incisors that is absolute control over lower incisors. (The proclination of lower incisors limits the forward displacement of mandible thereby reducing the scope of desired skeletal correction). It is highly beneficial and indicated in cases with severe incisor proclination where maximum orthopaedic correction is required.

Semi fixed twin block [11]
Compliance for removable twin block appliance wear is a major complication faced by orthodontists for successful functional correction. Therefore, in non-complaint cases this appliance proves to be of greater benefits. This appliance is a simple but versatile semi fixed Twin block appliance that ensures full time wear of the appliance that also keeps provision of possible modifications in different clinical scenarios.
Appliance design: Permanent maxillary molars are banded on both the sides, lingual sheath welded vertically on buccal and lingual aspects with their long axis parallel to each other. Bite registration is obtained in conventional technique and the cast along with the bite registration are then mounted on the hinge articulator. A 20-gauge hard stainless-steel wire is used to make double backs such that it fits the lingual sheath and the two ends of the double back should be opposite to each other.
The maxillary block is prepared as per standard twin block design at about 70 degrees to occlusal plane, the free ends of double backs are placed in vertical sheath and embedded into acrylic blocks. Lower blocks are prepared in conventional manner and can be cemented directly onto mandibular teeth. After completion of active phase same maxillary bands with lingual sheaths are used for making fixed incline plane. The phase of retention is continued till the occlusion settles in perfect harmony.
This appliance is fabricated easily without unnecessary laboratory procedures, it further reduces the dependence on compliance of patients. The ease of bracket placement in the anterior region reduces the treatment time significantly. Trimming of bit blocks for selective eruption of teeth is possible which would have been difficult in other fixed twin block cases.

Fixed twin block [12]
When compared to removable appliances fixed appliances do not rely on patients’ compliance. The fixed twin block system combine with conventional fixed appliance system provides for better means of arch development.
Individual fixed blocks can be customized on models prior to fitting in the mouth of the patient allowing space for Essix material. Buccal tube can be added to molars to allow attachment of wires.
Therefore, when used with fixed appliance treatment correction of overjet overbite and alignment of the labial segment may be facilitated with improved anchorage without undergoing any invasive procedure. This appliance provides the perfect integration of orthodontic and orthopedic therapy.
Appliance design: contains only acrylic bite blocks therefore this appliance is less bulky and it is easier to maintain oral hygiene.
This appliance is used along with fixed orthodontic treatment therefore aids in shorter treatment duration and there is less reliability on patient compliance. This appliance according to the study was successful in increasing the mandibular length significantly and is advised for use in uncooperative patients for favourable treatment outcomes.
Twin block with jackscrew for reactivation: [13]
Twin block appliance when used for overcoming a large overjet needs to be reactivated in stepwise manner to allow comfortable progress of treatment for correction of overjet, to achieve full edge to edge protrusive position or to attain overcorrection. Recent studies have suggested that the gradual increase, that is incremental advancement has had a more successful response during growth modification with lesser chances of incisor tipping which in unfavourable to the treatment outcome.
Reactivation or to progress with incremental increase of twin block requires time and unnecessary laboratory procedures with self-cure acrylic. Thus, the incorporation of jackscrew in the bite blocks allows easy reactivation and a better treatment control.
Appliance design: self-curing acrylic is added to one end of jackscrew up to the plastic separator forming a 70-degree angled plane on mesial surface of the block, the other end of the jackscrew is incorporated on the mesial surface of the upper block’s main body. Activation is done in slow gradual manner and can be used with class III or reverse twin block design. This is used in cases with large overjet that may need stepwise advancement. It reduces the need for remounting and extra lab procedure.
The advantages of this type of fabrication are ease of adjustment at the chair, accurate measurable adjustments that can be carried out unilaterally or bilaterally and requires no special screws or spacers. It also enhances patient tolerance and potential increase in the growth response of the mandible. The changes are reversible in cases of over advancement which is beneficial and trimming blocks in brachycephalic patients with deep bite is possible since the jackscrews are placed close to the maxillary dentition.

Magnetic twin block [14]
The role of magnets in Twin Block therapy is specifically to accelerate correction of arch relationships. The purpose of the magnets is to encourage increased occlusal contact on the bite blocks to maximize the favourable functional forces applied to correct the malocclusion. Two types of rare earth magnet (samarium-cobalt and neodymium-boron) have been used to examine the response to attracting magnetic forces in Twin Block treatment. Both are effective, but neodymium-boron delivers a greater force from a smaller magnet. Attracting magnets incorporated in occlusal inclined planes may be effective to maintain the forward mandibular posture when the patient is asleep. Patients who have magnets added to Twin Blocks during treatment reported increased occlusal contact by day and observe also that the blocks are in contact on waking up.
Animal experiments conducted have suggested that magnetic functional appliances have a greater mandibular growth response as compared to the non-magnetic appliances of similar designs. Similar experiments were conducted that incorporated magnetic appliance with adjustable screws for the advancement of maxilla that showed midfacial protraction with horizontal maxillary displacement and anterosuperior premaxillary rotation (Vardimon et al. 1989,1990).
Addition of attracting magnets to the inclined planes using the magnetic forces to achieve maximum orthopedic treatment response.
The use of attracting or repelling magnets is the first consideration. The advantages of using either can be considered, as for the attracting magnets the forces generated pulls the appliance closer and encourages the patient to occlude actively and consistently in forward position and may therefore accelerate progress by increasing the frequency and force of contact on the inclined planes.
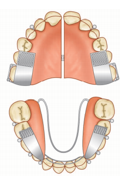
Twin block sagittal appliance [1]
Sagittal development is required when upper or lower incisors are retroclined with deep overbite. It is designed primarily for anteroposterior arch development by positioning two screws which are aligned anteroposteriorly in the palate. There is also allowance for some amount of oblique movements made possible by offsetting the angulation to obtain an additional component of the buccal segment expansion.
The positioning of the screws determines whether the appliance is made to move the upper anterior teeth labially or to move the move the upper posterior teeth distally. In cases with asymmetrical arch development, if more distal movement is required unilaterally the screw on one side may be activated more than the other.
It is also necessary to place the screws in the palate in horizontal plane and not inclined downward or anteriorly that may cause the appliance to ride down the anterior teeth thereby reducing the effectiveness of the procedure.
The lower twin block appliance also works o the same principle. The advancement of the lower labial segment is carried out by placing the lower curved screws in the canine region or by placing straight screws in the second premolar region to open up the space in the premolar area.

Twin block combined with Schwarz appliance[1] 1
Schwarz appliance have been used in the past to facilitate transverse development in both upper and lower arches during the mixed dentition period (Schwarz and Gratzinger, 1966). It can be therefore combined with twin block appliance to allow transverse development along with sagittal and vertical corrections if the arch relationship.
Addition of Screws in the upper and lower Twin Blocks allows independent control of arch width in both arches to improve anterior crowding or correct posterior crossbite in the mixed dentition stage. An upper transpalatal arch or lower Jackson design can also be used as an alternative to screws for the development of the maxillary and the mandibular arch respectively.
Twin block Crozat appliance[14]
Twin Block Crozat appliance (Crozat, 1920) is an useful alternative which can be used in adult treatment with minimum palatal and lingual coverage. This appliance has to be carefully adjusted to maintain the symmetry. The advantage of this twin block is that the palate free part that offers increased comfort and improved speech.
Twin block with spinner and occlusal rest [1]
Twin Blocks can be used to close an anterior open bite by applying an intrusive force to the posterior teeth. In some cases, occlusal rest has to be given on lower molars to prevent its eruption which would open the bite. The acrylic base plate can be extended over the cingulum of the upper and lower incisors before trimming the acrylic slightly to relieve contact with the incisors. This method allows the lingual flange serves to shield the incisors from the tongue which can be advantageous as it allows the incisors to erupt to reduce the anterior open bite.
Proclined upper incisors can be corrected using a labial bow to help reduce the anterior open bite. Tongue thrust can also be controlled by the addition of a spinner or tongue guard. In some cases, both may be indicated. A modified anterior inclined plane with a palate-free target can also be incorporated to control tongue thrust.
Invisible Esssix twin blocks with preformed blocks [1]
Invisible twin blocks are made with preformed occlusal blocks over the posterior teeth on the models enclosed in pressure moulded trays to fit over the teeth. This design is excellent for treatment of sleep apnea by posturing the mandible forward. This advances the tongue and increases the airway space. Appliances like these may be worn comfortably during the day to prevent accidents while driving. These concepts can also be combined with Invisalign to achieve simultaneous correction of arch relationship and alignment of anterior teeth.

Designer twin blocks [1]
It is important to give attention to individual patient needs, young patients like to be involved in choosing colour and design of the appliance. Designing of the appliance can be done in unlimited ways depending on the imagination of the designer. Orthodontic laboratories have the skills to meet the customization of every patient according to their want. It helps younger patient to be more compliant and take the treatment protocol appreciatively and enthusiastically.

Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Source of Funding
None.
References
- William J. Twin Block Functional Therapy-Applications In Dentofacial Orthopaedics. 3rd Edn.. . 2015. [Google Scholar]
- RAM, Bhad WA, UHD. Effectiveness of reverse twin block with lip pads-RME and face mask with RME in the early treatment of class III malocclusion. Prog Orthod. 2019;20(1). [Google Scholar] [Crossref]
- Harradine NW, Gale D. The effects of torque control spurs in twin-block appliances. Clin Orthod Res. 2000;3(4):202-9. [Google Scholar] [Crossref]
- Parkin HFNA, Mckeown PJ, Sandler. Comparison of 2 modifications of the twin block appliance in matched class II samples. Am J Orthod Dentofacial Orthop. 2001;119(6):572-7. [Google Scholar] [Crossref]
- Campbell C, Millett D, Kelly N, Cooke M, Cronin M. Frankel 2 appliance versus the Modified Twin Block appliance for Phase 1 treatment of Class II division 1 malocclusion in children and adolescents: A randomized clinical trial. Angle Orthod. 2020;90(2):202-8. [Google Scholar] [Crossref]
- Salloum E, DTM, Kelly N, McIntyre GT, Cronin MS. Soft tissue changes: a comparison between changes caused by the construction bite and by successful treatment with a modified Twin-block appliance. Eur J Orthod. 2018;40(5):512-8. [Google Scholar] [Crossref]
- Trenouth MJ, Desmond S. A randomized clinical trial of two alternatives designs of twin‑block appliance. J Orthod. 2012;39(1):17-24. [Google Scholar] [Crossref]
- Plas MCvd, Janssen KI, Pandis N, Livas C. Twin block appliance with acrylic capping does not have a significant inhibitory effect on lower incisor proclination. Angle Orthod. 2017;87(4):513-8. [Google Scholar] [Crossref]
- Dyer FMV, Mckeown HF, Sandler PJ. The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions. J Orthod. 2001;28(4):271-80. [Google Scholar] [Crossref]
- Tripathi T, Singh P, Rai P, Gupta. Mini-implant-supported twin-block appliance: An innovative modification. Niger J Clin Pract. 2019;22(3):432-8. [Google Scholar] [Crossref]
- Chandorikar H, Wasundhara A, Doshi UH, Chavan SJ. Versatile Twin‑block design for noncompliance class II correction. APOS Trends Orthod. 2016;6(5). [Google Scholar] [Crossref]
- Pattanaik S, Puvvula N, Mohammad N. Accelerating Treatment of Skeletal Class II Malocclusion using Fixed Twin Block Appliances. J Clin Pediatr Dent. 2018;11(2):146-50. [Google Scholar]
- Doshi UH, Bhad WA. A Simple Method for Twin Block Reactivation. JCO. 2011;6. [Google Scholar]
- Carmichael GJ, Banks PA, Chadwick SM. A modification to enable controlled progressive advancement of the Twin Block appliance. Br J Orthod. 1999;26(1):9-13. [Google Scholar] [Crossref]
- Abstract
- Introduction
- Twin block in Class III cases
- Twin Block to Control Incisor Inclination in Class II Malocclusion
- Modified twin block with torquing spurs [3]
- Modified twin block with torquing spurs and high pull headgear [4]
- Modified twin block with Southend clasp on lower central incisors [5], [6]
- Modified twin block with Southend clasp on upper and lower central incisors [7]
- Modified twin block with acrylic capping [8]
- Modified twin block for class II Div 2 [9]
- Modified twin block with mini implants [10]
- Semi fixed twin block [11]
- Fixed twin block [12]
- Twin block with jackscrew for reactivation: [13]
- Magnetic twin block [14]
- Twin block sagittal appliance [1]
- Twin block combined with Schwarz appliance[1] 1
- Twin block Crozat appliance[14]
- Twin block with spinner and occlusal rest [1]
- Invisible Esssix twin blocks with preformed blocks [1]
- Designer twin blocks [1]
- Conflicts of Interest
- Source of Funding
- References