
Introduction
Dr. Edward Hartley Angle introduced his E-Arch appliance1 in 1903, in which he used to use ligature wires which were made from a noble metal, i.e., Gold. Then, the Pin and tube appliance2 and the Ribbon Arch appliance3 needed pins to hold the wires in the bracket slot. Finally in 1929, Angle introduced his most widely accepted appliance, the Edgewise appliance,4, 5, 6, 7 which used ligature wires to secure the archwires in the bracket slot. In 1950s, Raymond P. Beggs, an Australian orthodontist, introduced a new technique called the Beggs Technique6 which was modified from Angle’s Ribbon arch technique and used light forces.
Another shift in the orthodontic technique happened when Larry Andrews presented the straight wire appliance.7 Rather than twisting wires to put teeth in the appropriate orientation with an edgewise bracket, Andrews' apparatus had the tip and torque incorporated into the brackets, thus the word "appliance prescription" was introduced. In theoretical knowledge, these pre-adjusted brackets finished the need to bend first, second, and third order bends each time the patient was advanced to the next wire. The straight wire appliance revolutionized orthodontics by making the section considerably more proficient.
From that point forward, numerous orthodontic organizations have fostered their own bracket systems with specific prescriptions, treatment philosophies, and mechanics. Nonetheless, they all had one common regular trademark – ligatures should be put around tie wings on brackets to hold archwires in the bracket slot.
Ligation and Materials Used
Since the inception of the orthodontic and introduction of various prescription of brackets, ligatures have in use. Stainless steel ligature wires and elastomeric ligatures have been in use mainly. The steel ligature wires are marketed in various dimensions ranging from 0.009” – 0.012” in diameter, ligated in a twisting manner using a Mathieu needle holder. In esthetic brackets, these steel ligatures are Teflon-coated for esthetic reasons. The advantage of these steel ligatures is that they retain their form and shape & do not corrode in the oral environment and also do not provide retention of plaque as they can be easily cleaned. Drawbacks of using a steel ligature may include that it is time consuming and tiresome for the operator. Harradine8 found that the use of wire ligatures added almost 12 minutes to the time needed to remove and replace two archwires. Careful tucking in of the ends of the cut ligature is necessary to avoid any trauma to the surrounding soft tissue.
Another milestone in the field of orthodontics was the introduction of the elastomeric ligatures in the 1970s. They are easier and quicker to place but in maloccluded teeth, they fail to provide full engagement of archwire into the bracket slot. They have a drawback that they have been shown to increase friction in the sliding mechanics and increase the resistance to movement.9, 10 Elastic ligatures undergoes force decay and permanent deformation in shape. They also increase plaque accumulation and also gets stained permanently due to the pigments present in the food.
Properties of an Ideal Orthodontic Ligation System
Regardless of the type of bracket and ligation used, there are several desirable properties for an ideal orthodontic ligation system.
Secure and robust ligation
Secure, full archwire engagement maximizes the potential long range of action of modern low modulus wires and minimizes the need to regain control of teeth where full engagement is lost during treatment.
Full bracket engagement
Full archwire engagement into the bracket slot is desirable to attain full expression of torque particularly at finishing stages of treatment.
Self-Ligating Brackets
As the name suggests, self-ligating brackets do not use ligature wires or elastic ligatures to engage archwires into their bracket slots. Rather they have their own locking mechanics incorporated into the bracket itself.
Stainless steel ligatures apply high force, and electrometric ligatures apply very high forces resulting in high friction between the archwire and the bracket slot. This increases the resistance to tooth movement during sliding mechanics with conventionally ligated brackets. Self-ligating brackets by minimizing the normal force caused by ligation decreases the resistance to sliding. There are essentially two main types of self-ligating bracket, depending on the design of the locking mechanism, the dimensions of the slot, and the dimensions of the archwires11 –
Active Brackets – The locking mechanism generally consists of a flexible but resilient clip that can actively engage wire into the bracket slot once the archwire reaches a certain size or deflection. E.g., Quick, Forestadent Ltd, SPEED, Strite Industries.
Passive Brackets – The slot is locked or shut with a rigid locking mechanism. Once it is engaged, the bracket is effectively turned into a tube, ideally allowing archwires to slide freely within the tube. E.g., Damon System, Ormco Corporation, Discovery SL, Dentaurum Ltd.,
The first design of self-ligating brackets was introduced in 1930 by Charles E. Boyd and since then there is no looking back. In this article, various self-ligating brackets have been described.
Boyd band bracket (Figure 1)
The first patent for self-ligating attachments, the Boyd Band Brackets was filed by Charles E. Boyd in 1930. The production was abandoned because the design proved to be too expensive and bulky to be commercially viable.
Russell lock attachment (Figure 2)
The first self-ligating bracket, the Russell attachment, was developed by a New York orthodontic pioneer, Dr. Jacob Stolzenberg, in the 1935.12 This bracket had a flat-head screw seated snugly in a circular, threaded opening in the face of the bracket. For the orthodontist, archwire changes were quick and simple. Loosening allowed bodily translation on a round wire, while tightening facilitated root torquing with a rectangular or square wire.
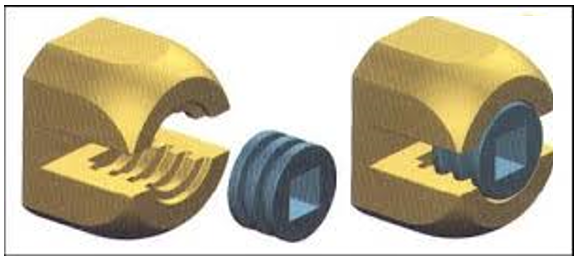
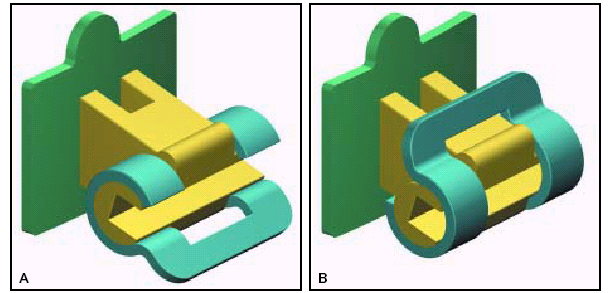
EdgeLok (Ormco) appliance (Figure 3)
In 1971, Dr. Jim Wildman of Eugene, Oregon, developed the EdgeLok bracket, which had a round body with a rigid labial sliding cap.13 When the cap was closed over the archwire with finger pressure, the bracket slot was converted to a tube. The EdgeLok was the first passive self-ligating bracket, and the first to enjoy any sort of commercial success.
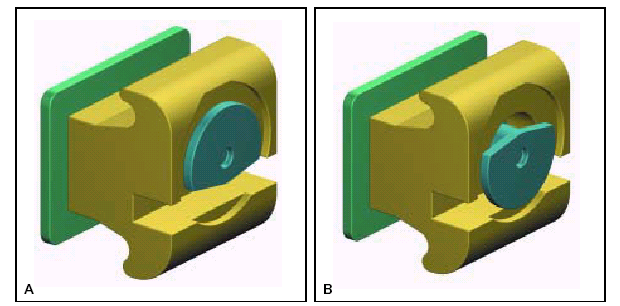
Mobil lock (Forestadent) (Figure 4)
A similar bracket, designed by Dr. Franz Sander of Ulm, Germany, was introduced in 1980.14 The Mobil-lock required a special tool to rotate the semi-circular labial disk into the open or closed position. As with the EdgeLok, the passive outer wall transformed the bracket slot into a tube that loosely contained the archwire. Perhaps because of the simultaneous introduction of elastomeric ligatures, however, neither the EdgeLok nor the Mobil-lock gained much of a following.
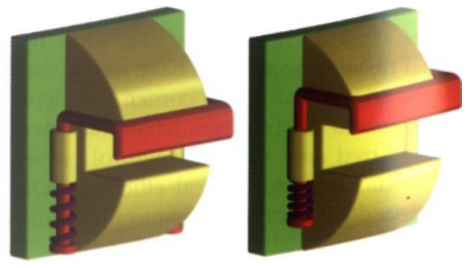
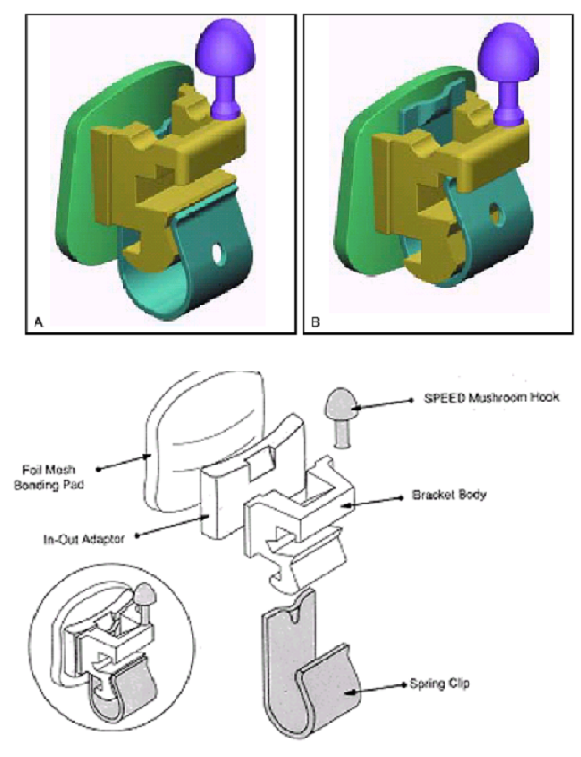
Speed appliance (Strite Industries) (Figure 5)
Hanson in 1975, combined Angle’s Edgewise appliance with his own concept of developing both a dynamic and self ligating appliance.15 This resulted in a spring – loaded, self – adjusting ligatureless design that possessed the unique quality of retaining and actively influencing control of the arch wire within the arch wire slot. This design is known as SPEED appliance (Strite Industrie Ltd., Ontario, Canada). In the ongoing quest for perfection, the SPEED appliance has undergone numerous refinements since its introduction in 1980.
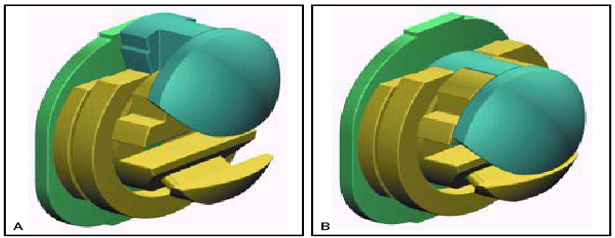
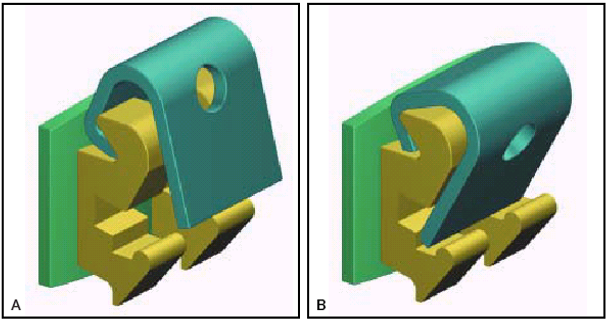
Activa bracket (“A” Company) (Figure 6)
In 1986, the self-ligating Activa bracket, designed by Dr. Erwin Pletcher, offered another alternative.16 The Activa bracket had an inflexible, curved arm that rotated occluso-gingivally around the cylindrical bracket body. As with the EdgeLok bracket, the passive configuration of the Activa bracket limited its interplay with the archwire. Drawbacks such as the ease with which patients could open the bracket and a large mesio-distal bracket width eventually led to its commercial demise.
Time bracket (Adenta) (Figure 7)
In 1995, another self-ligating model entered the marketplace. Designed by Dr. Wolfgang Heiser of Innsbruck, Austria, the Time bracket is similar in appearance to the SPEED bracket but its design and mode of action are significantly different.14 About the size of a conventional bracket, the Time features a rigid, curved arm that wraps occluso-gingivally around the labial aspect of the bracket body. The stiffness of the bracket arm prevents any substantial interaction with the archwire, thereby rendering Time a passive bracket.
Damon SL bracket (“A” Company) (Figure 8)
In 1996, the Damon SL bracket was introduced. 17, 18 This design was passive, and because of problem with bulky slide and limited tooth contol, its commercial life span was short.
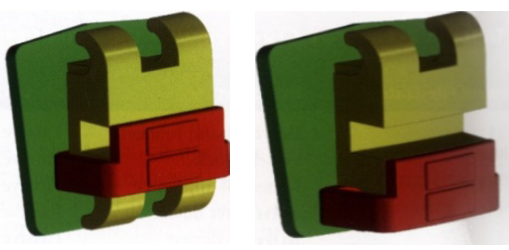
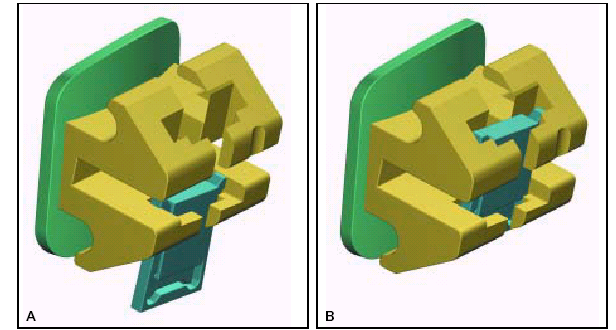
TwinLock bracket (Ormco) (Figure 9)
The TwinLock bracket, a second endeavour by Dr. Jim Wildman, was introduced in 1998.19 Its flat, rectangular slide, housed between the tie wings of an edgewise twin bracket, is moved occlusally into the slot-open position with a universal scaler. It then slides gingivally with finger pressure to entrap the archwire in a passive configuration.
Damon 2 bracket (“A” Company/ Ormco) (Figure 10)
Damon 2 brackets were introduced in 2000 to address the imperfections of Damon SL.17, 18 They retained the same vertical slide action and U-shaped spring to control opening and closing, but placed the slide within the shelter of the tie wings. However, the brackets were not immediately and consistently very easy to open and this aspect of functionality is important to the new user.

In ovation bracket (GAC) (Figure 11)
It is the first twin bracket with active clip to be introduced by Micheal C. Alpern in the year 2000. 14 They are similar to the SPEED bracket in conception and design, but are of a twin configuration. Bracket is manufactured with metal injection moulding. Active clip is made from cobalt chromium alloy which makes it highly resistant to fracture.

In ovation – R bracket (GAC) (Figure 12)
In 2002, smaller brackets for the anterior teeth became available – In-Ovation R (Reduced, referring to the reduced bracket width) and this narrower width was effective in terms of greater interbracket span. 14 The bracket subsequently became known as System R. They are a successful design, but some relatively minor disadvantages in bracket handling were initially apparent. Excess composite at the gingival aspect of brackets in the lower arch can be difficult to see and may also hinder opening. Similarly, lacebacks, underties, and elastomerics placed behind the archwire are competing for space with the bracket clip.

Philippe appliance (Forestadent) (Figure 13)
First described by Macchi et al in 2002, the first self-ligating lingual bracket can be bonded directly on the tooth surface. Since they do not have slots, only first and second order movements are possible.

Oyster ESL bracket (Figure 14 )
It is a passive self-ligating bracket system. Oyster ESL was developed to add esthetics. It was an alternative to self-ligating metal brackets and substitute for the traditional composite brackets. The bracket is made from fibreglass reinforced composite polymer. The materials that the Oyster ESL contains of is Polycarbonate (70%) and Polyethylene Terephthalate (30%).
Smartclip brackets (3M Unitek) (Figure 15)
It is a passive self-ligating bracket system. The integral nickel-titanium clip permits easy and simple archwire insertion and removal, yet hold the archwire with a pre-programmed force that avoids unintentional disengagement. 20

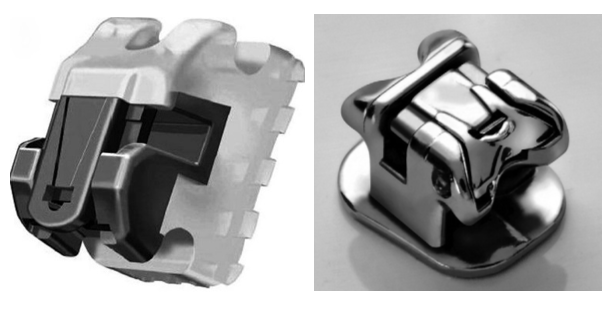
Damon 3 and damon 3MX brackets (Ormco) (Figure 16)
Damon 3 and Damon 3 MX brackets have a different location and action of the retaining spring, and this has produced a very easy and secure mechanism for opening and closing. In addition, Damon 3 brackets are semi-esthetic. The recently launched all-metal Damon D3 MX bracket has clearly benefited from manufacturing and clinical experience with previous Damon brackets.14


Conclusion
Currently available self-ligating brackets offer the very valuable combination of extremely low friction and secure full bracket engagement and—at last—they are sufficiently robust and user-friendly to deliver most of the potential advantages of this type of bracket. The core advantages of self-ligation are now established and readily available. These developments offer the possibility of a significant reduction in average treatment times and maybe also in anchorage requirements, particularly in cases requiring large tooth movements. Evidence of better treatment effectiveness exists but is incomplete. While further refinements are desirable and further studies essential, current brackets appear able to deliver measurable benefit with good robustness and ease of use.