- Visibility 166 Views
- Downloads 9 Downloads
- DOI 10.18231/j.ijodr.2020.051
-
CrossMark

Forsus fixed functional appliance therapy for dentoalveolar and profile correction- A case report
Introduction
Forsus fixed functional appliance is very effective in patients in whom growth has either completed or is either on the verge of completion. The successful use of this appliance in the treatment of skeletal Class II malocclusion is based upon factors such as; age of patient, compliance of the patient and other case selection criteria. Dentofacial orthopedic treatment can significantly alter and improve facial appearance in addition to correcting irregularity of the teeth. Functional appliances may be defined as orthodontic appliances that use the forces generated by the muscles to achieve dental and skeletal changes.[1], [2] These appliances have been used in clinical orthodontics for a long time and are extensively featured in the literature.[3], [4] Their effect is produced from the forces generated by the stretching of the muscles.[5] It is a commonly used functional appliance partly due to its acceptability by patients (Chadwick et al., 1998).[6] The muscles and soft tissues are stretched with the generated pressure transmitted to the skeletal and dental structures potentially resulting in skeletal growth modification and tooth movement [6] Management of class II malocclusion by growth modulation in adolescent patients is one of the most debated topics in orthodontics. Lack of compliance in adolescent population has been a major concern of healthcare providers. Every orthodontist appreciates the seriousness of compliance.
Noncompliance has been a major concern for orthodontists since more than 40 years.[7] However, predicting compliance before treatment may be difficult. Fixed appliance for class II correction requires minimal patient cooperation and they can be grouped into three categories based upon their mode of action.[8]
Rigid fixed functional orthopedic appliance viz herbst and its modifications.
Fixed maxillary appliances viz pendulum appliance. Apply class I force within maxilla. The resultant orthopedic and orthodontic effects are within the maxillary arch.
Interarch spring force delivery system viz Jasper Jumper, Forsus.
Management of class II malocclusion has wide spectrum of options. Since this patient presented with completed growth, it was decided to treat her with Forsus Fixed appliance therapy which promoted major dento-alveolar changes and minor but definite skeletal changes as well. We could not use a rigid fixed functional appliance viz herbst, as we do not have the laboratory facility to fabricate herbst appliance. Hence, we decided to use flexible fixed functional appliance - Forsus.
Case Report
Extra-oral examination
A young female patient, aged 18 years 4 months, sought an orthodontic evaluation with a chief complaint of forwardly placed upper front teeth and also backwardly placed lower jaw. On Extra-oral examination, the patient had a convex profile, grossly symmetrical face on both sides with a retruded chin, competent lips, moderately deep mentolabial sulcus and an average Nasolabial Angle, a Leptoprosopic facial form, Dolicocephalic head form, Average width of nose and mouth, minimal buccal corridor space, a consonant smile arc and posterior divergence of face. Patient showed presence of incompetent lips and increased strain of lips. The patient had no relevant prenatal, natal, postnatal history, history of habits or a family history. On Smiling, there was excessive show of maxillary anterior teeth. The patient also had a toothy smile

Intra-oral examination
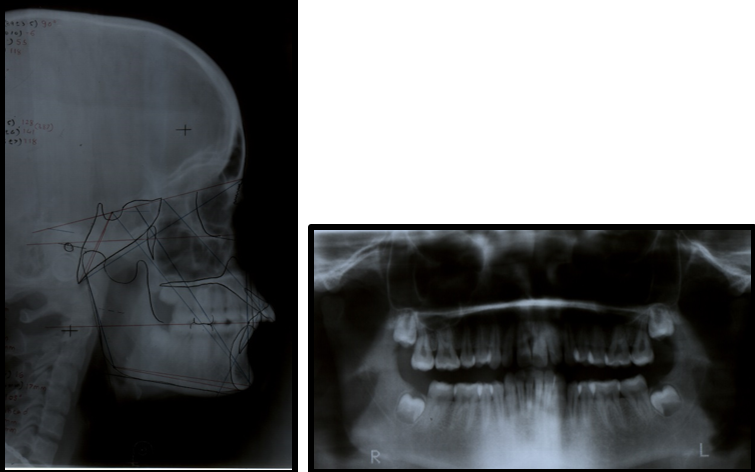
Intraoral examination on frontal view shows presence of a deep overbite, on side view the patient shows the presence of Class II div 1 incisor relationship, an end on canine relationship on both sides and an end on molar relationship on left side. Molar relation on right side was Class I. Patient has an overjet of 7 mm and an overbite of 5mm. There is spacing in upper anterior region and moderate crowding in lower anterior region. The upper and lower arch shows the presence of a “U” shaped arch form. OPG of the patient shows presence of all four 3rd molars in a developing stage. Lateral cephalogram is clearly indicative of a proclined upper and lower anterior teeth and a recessive lower jaw.

|
Parameters |
Pre- treatment |
|
SNA |
83° |
|
SNB |
78° |
|
ANB |
5° |
|
WITS |
5mm |
|
Max. Length |
75mm |
|
Man. Length |
98mm |
|
IMPA |
97° |
|
Nasolabial Angle |
93° |
|
U1 TO NA Degrees |
35° |
|
U1 TO NA mm |
8mm |
|
L1 TO NB Degrees |
30° |
|
L1 TO NB mm |
5mm |
|
U1/L1 Angle |
103° |
|
Saddle Angle |
130° |
|
Articular angle |
154° |
|
Gonial angle |
143° |
|
FMA |
24° |
|
Y AXIS |
69° |
Cephalometric evaluation
Steiners analysis shows an average maxilla and a retrognathic mandible, Class II Skeletal pattern, an Average to Horizontal growth pattern, proclined maxillary and mandibular anterior teeth, forwardly placed maxillary and mandibular anterior teeth and protrusive upper and lower lips
Tweeds analysis shows a Horizontal growth pattern and proclined mandibular incisors
Wits appraisal shows AO ahead of BO by 5 mm indicating Skeletal Class II pattern
Ricketts analysis shows a retrognathic mandible, retropositioned condyles and proclined mandibular anteriors
McNamara analysis shows an average maxilla, retrognathic mandible, a horizontal growth pattern, increased lower anterior facial height and proclined mandibular incisors
Rakosi Jaraback analysis shows a Horizontal growth pattern and proclined maxillary and mandibular incisors
Holdaway soft tissue analysis shows increased maxillary and mandibular sulcus depth and increased strain of lips
Downs analysis shows a retropositioned chin, a Class II Skeletal pattern, a horizontal growth pattern and proclined maxillary and mandibular anterior teeth
Diagnosis
This 18 year 4 months old female patient was diagnosed with Angle’s Class II div 1 malocclusion with an average maxilla, retrognathic mandible and a horizontal growth pattern, increased overjet and overbite, proclined upper and lower incisors, spaces in upper anterior region and crowding in lower anterior region, deep mentolabial sulcus and protrusive upper and lower lips, increased display of upper anterior teeth, incompetent lips and increased lip strain.
List of problems
Retrognathic mandible
Excessive display of upper anterior teeth
Spacing in upper anterior region
Crowding in lower anterior region
Proclined upper and lower anterior teeth
Increased overjet and overbite
Deep mentolabial sulcus
Deep curve of spee
Class II Division 1 Incisor relationship
End on Canine relationship bilaterally
End on Molar relationship on left side
Incompetant lips
Increased lip strain
Treatment Objectives
To correct retrognathic mandible
To reduce the excessive display of upper anterior teeth
To correct spacing in upper anterior region
To correct crowding in lower anterior region
To correct proclination of upper and lower anteriors
To correct overjet and overbite
To correct a deep mentolabial sulcus
To correct a deep curve of spee
To correct the incompetent lips
To correct the increased lip strain
To achieve a Class I Incisor relationship
To achieve a Class I Canine relationship bilaterally
To achieve a Class I Molar relationship bilaterally
To achieve a pleasing smile and a pleasing profile
Treatment Plan
To change the class II relation to class I without any premolar extraction, it was decided to treat this patient with fixed functional appliance Forsus (3M Unitek) in conjunction with preadjusted edgewise appliance in single phase. A 0.022" slot MBT prescription was used.

Treatment Alternatives
Treatment alternatives included either fixed Twinblock appliance therapy, Extraction of maxillary premolars with fixed appliance therapy or Orthognathic surgery. Option of fixed Twinblock was eliminated as the patient was already well beyond her growing age. Moreover the excessive bulk of the appliance was the reason why it wasn’t chosen. Extraction of upper premolars and ending the case in a Class II molar relation could be another option to improve the excessive display of upper anterior teeth, however this option was also eliminated because the fault was in the mandible, not maxilla and on VTO the patient showed improved profile and reduced prominence of upper front teeth, hence we decided to not extract the maxillary first premolars and treat the patient with a non- extraction protocol. Orthognathic surgery was the third and best option, however the patient refused it, so we decided to treat the case with Forsus Fixed appliance therapy which bought about more of dentoalveolar changes and less of skeletal changes given the patients age. The patient was informed about the compromised results as surgery was the best option in her case.
Treatment Progress
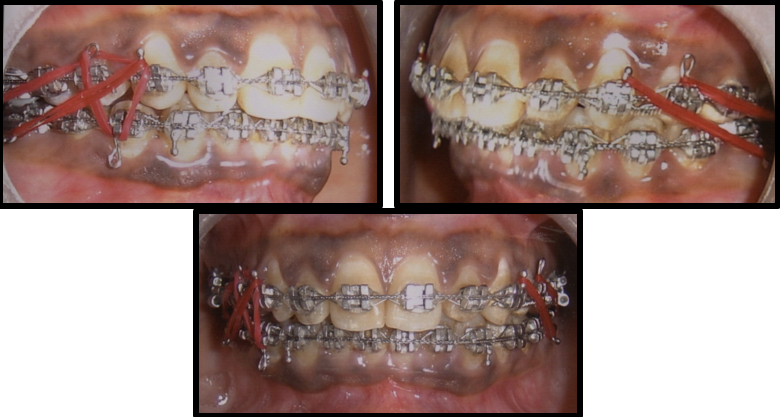
After complete banding and bonding, leveling and aligning were done in both the upper and lower arch with 0.012”, 0.014”, 0.016”, 0.018”, 0.020” NiTi arch wires following sequence ‘A’ of MBT. After 6 months of alignment and leveling NiTi round wires were discontinued. Reverse curve of spee in the lower arch and exaggerated curve of spee in the upper arch was incorporated in the heavy archwires to prevent the excessive bite deepening during retraction process and also to maintain the normal overjet and overbite. Individually both the arches were consolidated from molar to molar with figure of eight ligature tie and active bend back was placed in the archwire distal to the molar tube. Additional labial root torque was built into the anterior segment of lower archwire. The duration of pre-functional phase of treatment was 6 months. Then Forsus appliance was inserted. After two visits, a crimp was added for activation on left side of Forsus appliance for increased sagittal correction on left side and also for midline correction. Forsus was used for 12 months, a little longer than usual recommended duration. The occlusion was slightly overcorrected to class I, then Forsus was removed. Final finishing and detailing of occlusion were done which took about 4 months of time. Finally light settling elastics were given with rectangular steel wires in lower arch and 0.012” light NiTi wire in upper arch for settling, finishing, detailing and proper intercuspation. [9] After 18 months of treatment, the fixed appliance was debonded, a fixed lingual bonded retainer was bonded in the lower anterior region and wrap around retainer was fabricated for the upper arch.
Treatment Results
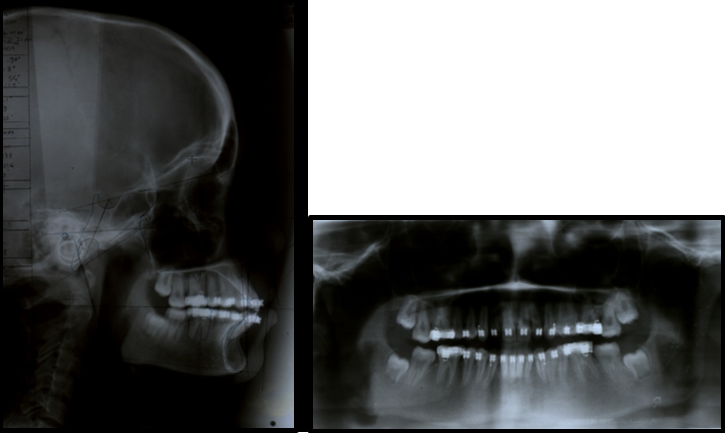
All of the original treatment objectives were achieved. The retrognathic mandible was changed to be more Orthognathic. The excessive display of upper anterior teeth was reduced. Spacing in the upper arch was closed and crowding in mandibular anterior teeth was unraveled The maxillary and mandibular arches were well aligned and coordinated without midline deviations. Normal overbite and overjet was achieved. Class I incisor relationship was achieved and Class I canine and molar relationship was achieved bilaterally. The chief complaint of forwardly placed upper front teeth and backwardly placed lower jaw was addressed. Lips changed from being incompetent to competent and lip strain reduced significantly at the end of treatment. Patient had a pleasant smile and a pleasant profile at the end of the treatment which continued over 18 months.
Discussion
Class II malocclusion might have any number of a combination of the skeletal and dental component. Hence, identifying and understanding the etiology and expression of Class II malocclusion and identifying differential diagnosis is helpful for its correction Fixed functional appliances have several well established advantages including the fact that it is well tolerated by patients and it can be used in the permanent dentition10. There are potential disadvantages such as the proclination of the lower incisors and development of posterior open bites. In this case, the treatment objectives were achieved largely due to good patient compliance. The patient's chief complaint was forwardly placed upper front teeth and a backwardly placed lower jaw. The selection of functional appliances is dependent upon several factors which can be categorized into patient factors, such as age and compliance, and clinical factors, such as preference/familiarity and laboratory facilities. The Forsus fixed functional appliance therapy resulted in an improvement in the patient's profile. It has been proved in the literature that fixed functional appliances do not produce long-term skeletal changes and most of their effects are dentoalveloar. [10] Pancherz [11] has emphasized the importance of good post treatment intercuspation for preventing the dental and skeletal relapse of class II correction. Teeth locked in stable class I intercuspation are more likely to transfer maxillary growth forces to mandible. [11] Bacetti [12] suggests that growth modulation done after the peak of growth spurt/decelerating phase of active growth spurt, results in greater skeletal contribution to molar correction. The following changes were seen with this single phase treatment using fixed orthodontic appliance and Forsus: ANB angle was reduced from 5 to 1°. Upper incisor inclination with respect to palatal plane was reduced from 120 to 107°.Upper incisor to NA angular value reduced from 35 degrees to 29 degrees and lower incisor to NB value reduced from 30 degrees to 24 degrees. The same value in millimeters reduced from 8mm to 2mm in maxillary arch and from 5mm to 2mm in mandibular arch. Maxillomandibular plane angle was not significantly altered. Overjet was reduced from 7 to 2 mm and Overbite reduced from 5mm to 2mm. Occlusion was changed from Angle’s class II division 1 to normal class I occlusion. Convexity of facial profile was reduced. Successful results were obtained after the Forsus fixed functional therapy within 12 months of time. The overall treatment time was 18 months. After this active treatment phase, the profile of this 18 year 4 months old female patient improved significantly as seen in the post treatment Extra-oral photographs.
|
Parameters |
Post-treatment |
|
SNA |
81° |
|
SNB |
80° |
|
ANB |
1° |
|
WITS |
1mm |
|
Max. Length |
76mm |
|
Man. Length |
104mm |
|
IMPA |
97° |
|
Nasolabial Angle |
96° |
|
U1 TO NA Degrees |
29° |
|
U1 TO NA mm |
2mm |
|
L1 TO NB DEGREES |
24° |
|
L1 TO NB mm |
2mm |
|
U1/L1 ANGLE |
132° |
|
Saddle angle |
123° |
|
Articular angle |
145° |
|
Gonial angle |
132° |
|
FMA |
24° |
|
Y AXIS |
70° |



|
Parameters |
Pre- treatment |
Post-treatment |
|
SNA |
83° |
81° |
|
SNB |
78° |
80° |
|
ANB |
5° |
1° |
|
WITS |
5mm |
1mm |
|
Max. Length |
75mm |
76mm |
|
Man. Length |
98mm |
104mm |
|
IMPA |
97° |
97° |
|
Nasolabial Angle |
93° |
96° |
|
U1 TO NA degrees |
35° |
29° |
|
U1 TO NA mm |
8mm |
2mm |
|
L1 TO NB Degrees |
30° |
24° |
|
L1 TO NB mm |
5mm |
2mm |
|
U1/L1 ANGLE |
103° |
132° |
|
Saddle Angle |
130° |
123° |
|
Articular angle |
154° |
145° |
|
Gonial angle |
143° |
132° |
|
FMA |
24° |
24° |
|
Y AXIS |
69° |
70° |
Conclusion
Fixed functional appliance therapy is an effective way of treating skeletal Class II malocclusion by promoting both growth modification and encouraging dentoalveolar correction. The effect of “Forsus” fixed functional appliance is mostly dentoalveloar with small skeletal component. However, there are a number of situations where fixed functional appliances can be successfully used to correct Class II malocclusion. It is important that fixed functional appliances be used in growing patients to achieve maximum benefit. In spite of all the present controversies about the growth modulation or functional appliances, even today functional appliances can be very useful tool in managing a class II malocclusion.
Source of Funding
No financial support was received for the work within this manuscript.
Conflict of Interest
The authors declare they have no conflict of interest.
References
- W J Clark. The Twin Block technique. A functional orthopaedic appliance system. Am J Orthod Dentofac Orthop 1988. [Google Scholar]
- T M Graber, T Rakosi, A Petrovic. Dentofacial orthopedics with functional appliances. 1997. [Google Scholar]
- O Brien. The effectiveness of treatment of class II malocclusion with the Twin Block appliance: A randomised, controlled trial. Am J Orthod Dentofac Orthop 2003. [Google Scholar]
- O Brien. The effectiveness of treatment of class II malocclusion with the Twin Block appliance: A randomised, controlled trial. Part 2: Psychological effects. Am J Orthod Dentofac Orthop 2003. [Google Scholar]
- J. R. E. Mills. The Effect of Functional Appliances on the Skeletal Pattern. Br J Orthod 1991. [Google Scholar] [Crossref]
- G D Singh, M R Hodge. Bimaxillary morphometry of patients with Class II division 1 malocclusion treated with twin block appliances. Angle orthod 2002. [Google Scholar]
- B Annemieke, J Hoogstratan, B Prahl-Andresen. On the use of personality characteristics in predicting the compliance in orthodontic practice. Am J Orthod Dentofacial Orthop 2003. [Google Scholar]
- P Devincenzo John, Thomas M Graber, Robert L Vanarsdall, Katherine WL. Treatment options for sagittal correction in noncomplaint patients in orthodontics: Current principles and techniques. 2009. [Google Scholar]
- B Nelson, U Hägg, K Hansen, M Bendeus. A long-term follow-up study of Class II malocclusion correction after treatment with Class II elastics or fixed functional appliances. Am J Orthod Dentofac Orthop 2007. [Google Scholar] [Crossref]
- P Panigrahi, V Vineeth. Biomechanical Effects of Fixed Functional Appliance on Craniofacial Structures. Angle Orthod 2009. [Google Scholar] [Crossref]
- Hans Pancherz. The Modern Herbst Appliance. Dentofac Orthop Funct Appl 1997. [Google Scholar]
- T Baccetti, L Franchi, L R Toth, J A McNamara. Treatment timing for Twin-block therapy. Am J Orthod Dentofac Orthop 2000. [Google Scholar] [Crossref]