
Introduction
Conventional anchorage provides very limited options for anterior anchorage reinforcement during molar protraction, especially in the mandibular arch. It typically involves using the anterior teeth as the anchorage unit, but this is limited by these teeth’s relatively low combined root surface areas.1 Protraction of molars is easier in the maxilla than in the mandible owing to the relative abundance of trabecular bone in the former. The large amount of cortical bone and the surrounding powerful musculature in the posterior mandible adversely affect anteroposterior molar movement, which becomes even more difficult with time as the alveolar bone narrows.2 In lieu of surgical alveolar ridge augmentation, substantial reductions in alveolar height and width may severely limit mesial movement of the posterior teeth, especially in hypodontia cases (where the alveolus is hypoplastic) or long-standing edentulous sites (where it has atrophied).1
Molar protraction is also more difficult in adults than in children. Children and young adults have fewer periodontal and root resorption problems during space closure than do older adults. 2 This review article provides a brief idea on the assortment of treatment approaches for molar protraction.
Indications
Class I, II and III malocclusions with generalized spacing where overjet is minimal.
Class II molar relationship where mandibular is to be protracted.
Cases of Class I malocclusion Type 1 where first premolars extraction was done and after complete retraction, the extraction space is left in the maxillary arch
Cases of end on/full class II molar relation due to mandibular retrognathism where second premolars extraction were done to correct the molar relation.
Cases of class III molar relation, where the molar correction is to be done and also to correct the reverse overjet.
Anchorage loss during active orthodontic treatment.
Permanent molars lost due to decay wherein the 2nd molars are to be mesialized
Cases of vertical growth pattern, like skeletal open bite where mesializing the molars in the extracted space helps in bite closure.
Excessive lower anterior facial height.
Contraindications
Diagnostic criteria (Case Selection)
Cases with minimal overjet with extraction space not completely closed.
Straight profile where retraction of anterior teeth results in dishing in of face.
The permanent molars are tipped in the space of missing premolars and permanent molars.
When Class I canine relationship in both the arches are attained.
When the molar relation is class II and class III.
Pitchfork analysis is done to see the distance from first molar to incisors and the post treatment results of the same are compared. It determines how much the molar has mesialized in relation to the dentition and the maxillary and mandibular bases.
Biomechanics
Friction mechanics
In terms of space-closure mechanics, molar protraction is similar to canine retraction: the primary biomechanical considerations relate to the anteroposterior translatory displacement of teeth. The role of friction during sliding and deflection of the arch wire are two important concepts that need to be understood to plan efficient and effective space closure. These two factors if not controlled will lead to binding of the arch wire causing unwanted movements like mesial molar tipping. 3 This can result in protraction (mesial shunting) of the entire dental arch and incisor intrusion. This manifests as a reduction in overjet and overbite. 1

If there are signs of unfavourable incisor intrusion then add a bite-closing curve to the arch wire. If incisor advancement and proclination occur, as a result of arch wire binding, then consider adding supplementary traction from the molars to the anterior teeth or arch wire hooks.
F- Force Applied, D – Distance b/w point of force application and COR, MTW – Molar tube width
Therefore, applying optimal force levels closer to the COR and using wider brackets can reduce frictional resistance during molar protraction. 2, 3
To reduce the friction between wire and molar tube, the ends of the wire should be rounded with a diamond bur and polished with a rubber wheel before insertion. 2
The second most important challenge faced during protraction is the deflection of arch wire. 3
F – Force applied, L – Inter-bracket span, AD – Arch wire dimension
If the molars are to be moved along a continuous arch wire, a 0.016 X 0.022-inch or 0.017 X 0.025-inch SS wire (in 0.018-inch slots) or 0.019 X 0.025-inch SS wire (in 0.022-inch slots) is recommended to avoid mesial tipping. Anchorage needs to be reinforced by 3/16- or 1/4-inch, medium Class II elastics between the mandibular second molars and maxillary canines (or lateral incisors). 2
Forces applied at the coronal level will tip molars mesially during protraction, especially if there is a vertical alveolar deficiency on the mesial aspect of the molar. This also tends to be worse if a second molar is not available or attached to help control the first molar alignment. 1 In the initial phase of protraction, the application of an elastic force from a mini-implant to the molar will generate an Mf as the force is applied above the CR of the molar.3 This results in mesial tipping due to the play between the bracket slot and the wire.

As molar tips mesially, arch wire contacts molar-tube edge, creating moment of couple (Mc) that uprights mesially tipped molar with decay of applied force.

With mesial displacement of the molar, the force will decrease in magnitude, due either to decay or relaxation of the applied force, thus reducing Mf. In this phase, when Mc is equal to Mf, the tooth will translate. Later, when Mc is greater than Mf, a significant amount of frictional resistance (primarily due to binding of the arch wire to the bracket slots) is generated at the wire-tube interface. This causes the centre of rotation to move occlusally between the molar tube and CR, resulting in root uprighting of the molar. 3, 2
Frictionless mechanics
If frictionless mechanics are preferred, a 0.017 X 0.025-inch SS wire with a closing loop can be used. A distal tip-back and toe-in should be made to avoid mesial tipping and mesio-lingual molar rotation. It is important to maintain the axial inclination of the molar by controlling the amount of activation of the loop. 2

During protraction, the force is applied buccal to the COR, which can cause mesio-lingual rotation. This can be prevented either by incorporating a toe-in bend in the arch wire or by attaching a lingual sheath in the molar and a lingual button in canines thereby incorporating an additional A-P force vector lingually.
Vertical molar control
During protraction, some premature contacts in the posterior segment or molar extrusion (because of mesial tipping) may affect the vertical dimensions of the face. In normal to low angle patients, molar extrusion is helpful to open the bite. In high-angle or skeletal open bite patients, however, molar extrusion needs to be controlled by careful mechanical application. In these cases, molar intrusion is achieved first followed by protraction mechanics. This can be effectively done with a posterior bite block or micro-implant anchorage mechanics.
Special Considerations while using TAD’s
The use of a posterior power arm, to apply traction at the molar furcation level, assists bodily molar movement and unidirectional space closure. involves placement of a double tube attachment on at least one molar per dental quadrant, then fabrication of a steel powerarm from a piece of rigid arch wire, e.g. 0.021 × 0.025 size. 1

A shallow posterior buccal sulcus depth may prevent initial placement of a power arm, especially on the terminal molar, but this can be added once sufficient mesial movement of the molar moves it into an area with more sulcus depth.
Techniques of molar protraction
Molar can be protracted by extraoral as well as the intraoral appliances. In intraoral techniques, molars can be protracted by friction and frictionless mechanics, intraoral elastics, temporary anchorage devices, removable and fixed appliances.
Extraoral Appliances
Facemask or reverse pull headgear3, 4, 5, 6, 7
Delaire, Verdon and Floor used a facial mask to protract the maxilla. In 1960’s Delaire and others revived the interest in using facemask for maxillary protraction. Petit later in 1983 modified the basic concept by increasing the force and decreasing the overall treatment time. In case of skeletal Class III malocclusion whole maxilla along with molars can be protracted.

Modified Protraction headgear9
This is introduced by Nanda in 1980. The study shows that the use of appliance for 4-8 months can displace the maxilla 1-3 mm and themaxillary dentition by 1-4mm. Maxillarymodified protraction headgear (MMPH)can be used effectively in Class III patientswith retrognathic maxilla and anterior open bite tendency.

Intraoral Appliances
Mandibular protraction appliance (MPA)10, 11, 12, 13
Is a recently developed noncompliant rigid fixed functional appliance that holds the mandible anteriorly and corrects the Class II anteroposterior discrepancy. This appliance is basically used for mandibular molar protraction. There are four types of mandibular protraction appliance, these are MPA I, II, III and IV which are used for correction of class II malocclusion.
Tandem Traction Bow Appliance (TTBM)15
Was designed in the year 1999 by Chun et al for the correction of class III malocclusion.
This intraoral appliance was designed for esthetic reasons and patient’s comfort.
TTBM helps in the mesialization of maxilla as well as maxillary dentition in cases of class III malocclusions.

NiTi closed coil springs and Elastomeric chains17
Are used for space closure. The anchorage unit is formed from premolar to premolar and the molars are protracted with NiTi closed coil springs. This is indicated in Class I, II and III malocclusions with generalized spacing where overjet is minimal and in cases of Class I malocclusion Type 1 where first premolars extraction were done and after complete retraction, the extraction space is left in the maxillary arch.
Figure 6
Left (A) and right (B) Springs are attached to crimpable ball hook on arch wire just distal to upper canine at one end and the hook on upper first molar bracket assembly at other end. 17

Class II intermaxillary elastics18
Can be used for the protraction of molars. Class II intermaxillary elastics are used for protraction of mandibular molars.
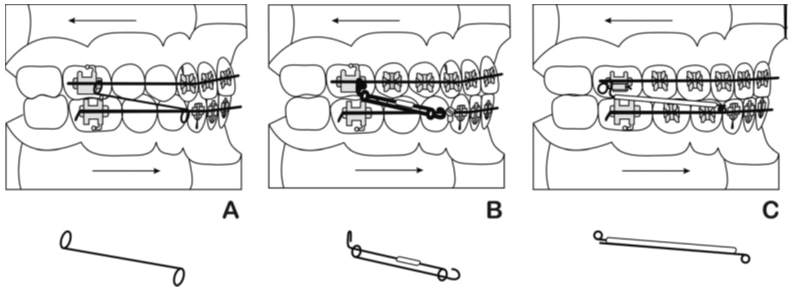
Cherry loop 21
Is made of resilient 0.17 x 0.25 stainless steel wire. This wire is sufficiently elastic and slides smoothly inside a 0.22x0.28” molar tube. It is bent using a pair of Rouland pliers. The design of the loop being a large-diameter round loop with a height of 8–9 mm; width - 8 mm which is open at the occlusal end by 3–4 mm. This is to avoid bite stress and to minimize the deformation of the wire.
The position of the loop must be kept at one-half the distance separating the bracket of the lower first bicuspid from the molar tube of the first molar. A tip-back bend of 200 is given to the distal leg. As the molar will protract, the loop must be brought to one-half the distance. This can be achieved by shortening the wire with a V bend placed distal to the canine tooth. The activation of the loop occurs in two phases.

Running loop 22
Is a simple and efficient method of closing the space without mesial or lingual tipping and rotation. This is done by facilitating simultaneous uprighting and mesial movement of molars commonly referred to as walking of molars. It is made up of 0.018 x 0.025 stainless steel wire. Its helical running loop is wound to the outside with an external diameter of 3 mm. The distance between the mesial end of the buccal tube and the running loop should be maintained at 5 mm, an effective tip-back of 20° to 30° should be given according to the amount of mesial tipping of molars, and a slight toe-in is necessary to prevent mesio-lingual rotation of the molars.

T loop 23
Was designed by Burstone in the year 1976. This was later modified by Hoenigl et al24 (1995) by increasing the length of vertical arm and decreasing the force by 230-256 grams. T loop can be fabricated by 0.016x0.022 SS wire or 0.017 x 0.025 TMA wire. The length of T loop is 10 mm with 2 mm height and a mesial leg of 4 mm and a distal leg of 5 mm. The activation of T loop causes the translation movement of teeth by simultaneous uprighting and mesial movement of molars.
Mini-implants 25
Are effective in providing absolute anchorage for 2nd molar protraction and thereby preventing unwanted side effects in the anterior segment. Technological advances in orthodontics are primarily aimed at reducing treatment time, reducing postoperative pain, and enhancing periodontal health. Treatment time for space closure by 2nd molar protraction in adults ranges from 2 to 4 years. 26 One end of elastomeric chains or NiTi coil springs are attached to mini-implants and the other end at the molar to be protracted.
Corticotomy assisted molar protraction27
Periodontally accelerated osteogenic orthodontics (PAOO) is a modified approach involving corticotomies and particulate bone allografts, which has been reported to enhance the rate of tooth movement by increasing alveolar bone turnover and reducing bone density. 28 PAOO approach is used for bilateral molar protraction using mini-screws for anchorage.
Conclusion
Keeping in mind the various methods through which one can approach Molar protraction, one should always check on the ease of the procedure avoiding dexterity for the clinician and also patient compliance must be seen. Over all the efficiency lies in the hand of the clinician more than the technique itself.